Why Unreacted MDI Remains in Foam
Spray foam insulation is created by combining two liquid components—a resin side containing polyols and a hardener side containing isocyanates (MDI). When these are mixed in precise ratios and sprayed, they undergo a rapid exothermic chemical reaction that transforms the liquids into solid foam. Ideally, this reaction runs to completion, with nearly all the isocyanate reacting with the polyols and becoming chemically incorporated into the foam polymer structure.
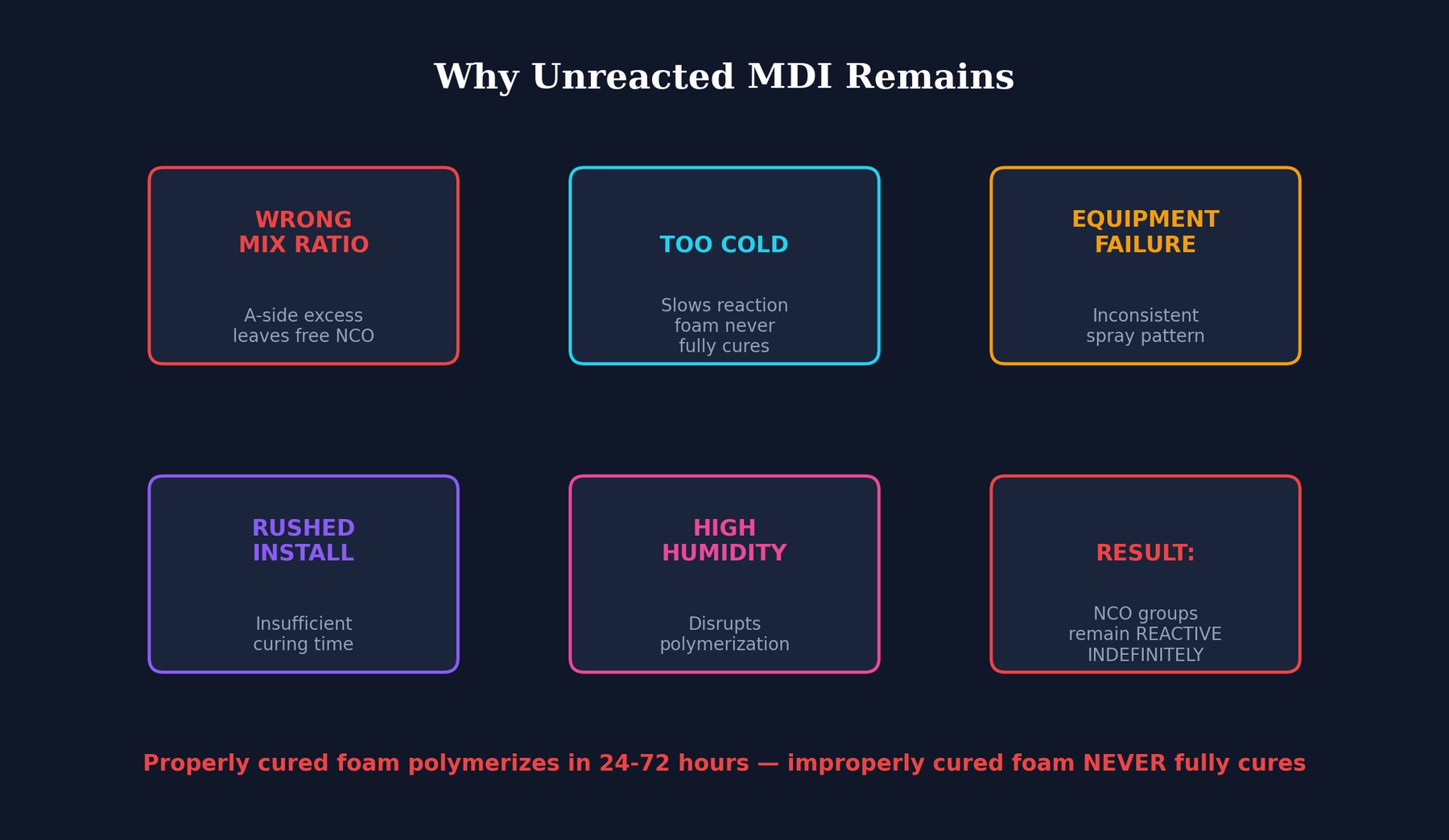
However, several common errors in installation can leave unreacted MDI (isocyanate) trapped in the foam:
- Wrong Mix Ratio: If the two components are not combined in the correct proportions, one side will be in excess after the other is depleted. An excess of isocyanate means unreacted MDI remains in the foam.
- Cold Temperatures: Isocyanate-polyol reactions are temperature-dependent. Cold ambient temperatures slow the reaction rate. If the foam cures in cold conditions, the reaction may not complete before the foam sets, trapping unreacted MDI.
- Equipment Failure: Spray foam equipment must maintain precise pressures, temperatures, and mixing ratios. Equipment malfunction—worn pumps, blocked lines, temperature controllers failing—leads to improper mixing and incomplete reactions.
- Rushed Installation: Some installers rush the application or apply foam in unsuitable conditions. Incomplete curing at the time the space is reoccupied means reactions are still ongoing in the walls.
- High Humidity: While some moisture is needed for certain foam formulations, excessive humidity can interfere with proper curing, leaving unreacted isocyanate.
Properly mixed and installed foam cures in approximately 24-72 hours. Improperly mixed foam may never fully cure—the unreacted MDI may remain in the foam indefinitely, continuing to off-gas over months or years.
Acute vs. Chronic Exposure: Why Chronic Is More Dangerous
MDI exposure can be acute or chronic, and understanding this distinction is crucial to understanding the silent danger of residential spray foam:
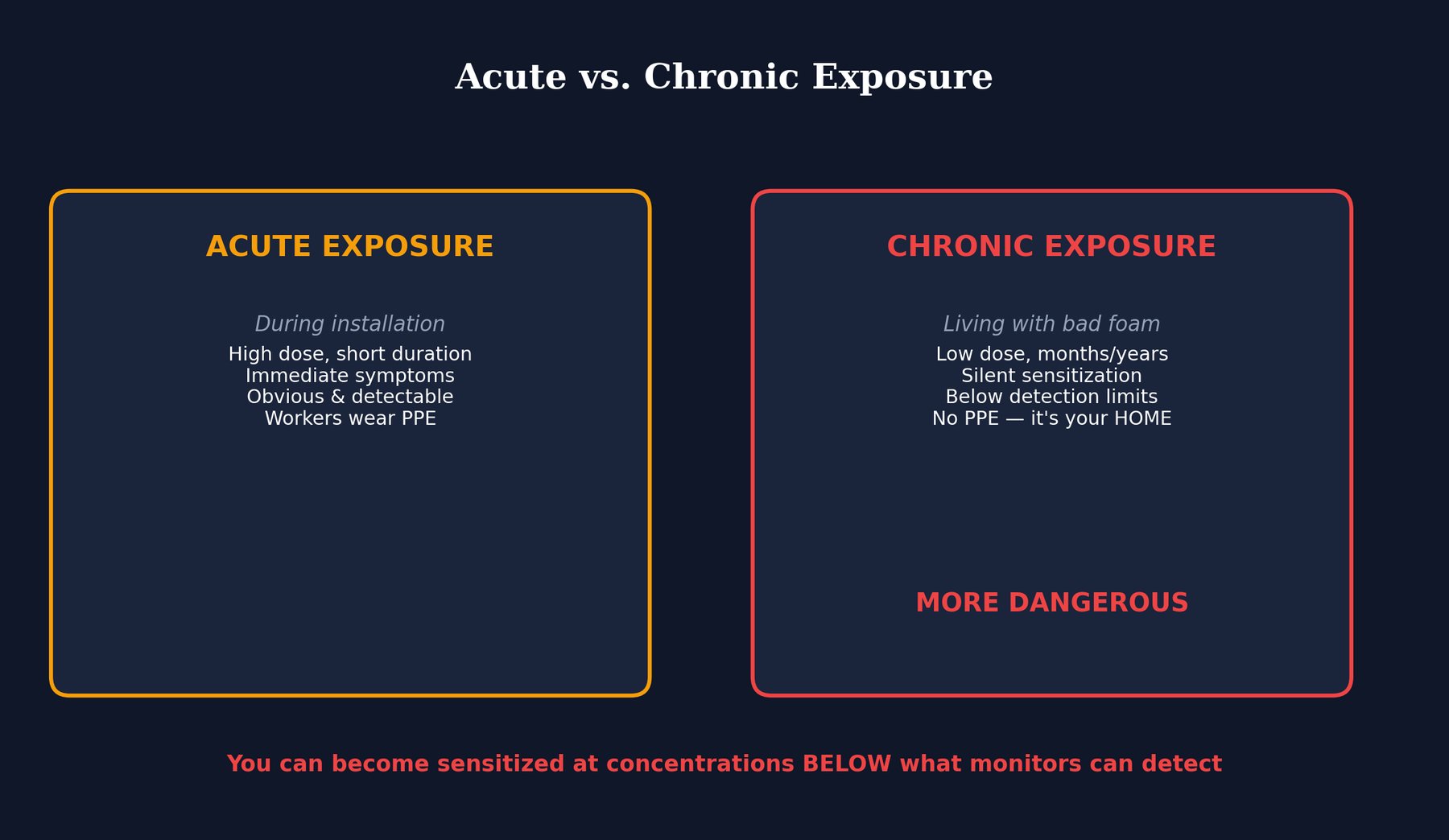
Acute Exposure
Acute exposure is high-dose exposure over a short period—what a foam installer experiences during spray application or immediately after. The symptoms are obvious and uncomfortable: respiratory distress, burning eyes and throat, coughing, wheezing. The exposed worker typically wears personal protective equipment (respirator, gloves, eye protection), and the exposure is time-limited (several hours of installation). After the acute exposure ends, the worker leaves the site and symptoms gradually resolve. Medical attention may be sought, and the cause of illness is usually recognized.
Chronic Exposure
Chronic exposure is low-dose exposure over months or years—what happens to a homeowner living in a house with improperly installed foam. The exposure is subtle: low-level isocyanate vapor continuously off-gassing from the foam in the walls and crawlspace. The exposed person doesn't wear protective equipment because they don't know they're being exposed. The exposure is continuous, 24/7, while they sleep, eat, work in the home. The doses are below levels that cause immediate, obvious symptoms in most people. The exposure is ongoing, not time-limited.
This chronicity is why residential exposure can be more dangerous than acute occupational exposure. The human immune system has remarkable tolerance for occasional challenges, but continuous, relentless exposure at low levels triggers different, often more permanent, responses.
Silent Sensitization: How Your Immune System Is Reprogrammed

The most insidious aspect of chronic MDI exposure is that it can cause permanent immune sensitization without obvious symptoms. Here's the mechanism:
Protein Binding
When MDI vapor enters the lungs, it immediately reacts with proteins—both in the lungs and in the bloodstream. MDI is an electrophile that covalently bonds to lysine residues on proteins, particularly albumin (a major blood protein). This creates MDI-protein conjugates—neoantigens that the immune system has never seen before.
Immune Recognition
The immune system's job is to recognize foreign substances and mount appropriate defenses. When it encounters these MDI-protein conjugates, it recognizes them as foreign invaders. But unlike bacteria or viruses, the immune system hasn't seen MDI before. It treats it as a novel threat requiring a specific immune response.
Antibody Production and Memory Cell Formation
The immune system produces two types of antibodies against MDI-protein conjugates: IgE antibodies (responsible for immediate allergic reactions) and IgG antibodies (responsible for longer-term immunity). More importantly, the immune system creates memory B cells and memory T cells—long-lived immune cells programmed to recognize MDI and mount a rapid, aggressive response whenever MDI is encountered in the future.
Permanent Sensitization
This sensitization is permanent. Once formed, memory immune cells persist in your body for years or decades. If you become sensitized to MDI through chronic low-dose exposure in your home, you will be sensitized for life. Any future exposure to MDI—whether from new foam installation elsewhere, from occupational exposure, or even from accidental exposure—will trigger a rapid, severe allergic response from your primed immune system.
No Safe Threshold for Sensitized Individuals
For a sensitized person, there is no "safe" level of MDI exposure. Even sub-ppb levels (below the detection limits of standard monitors) can trigger symptoms because the immune system is pre-programmed to recognize and respond aggressively to MDI at any concentration.
The Detection Gap: Why Your Air Monitor Says "Safe" While Your Immune System Is Being Reprogrammed
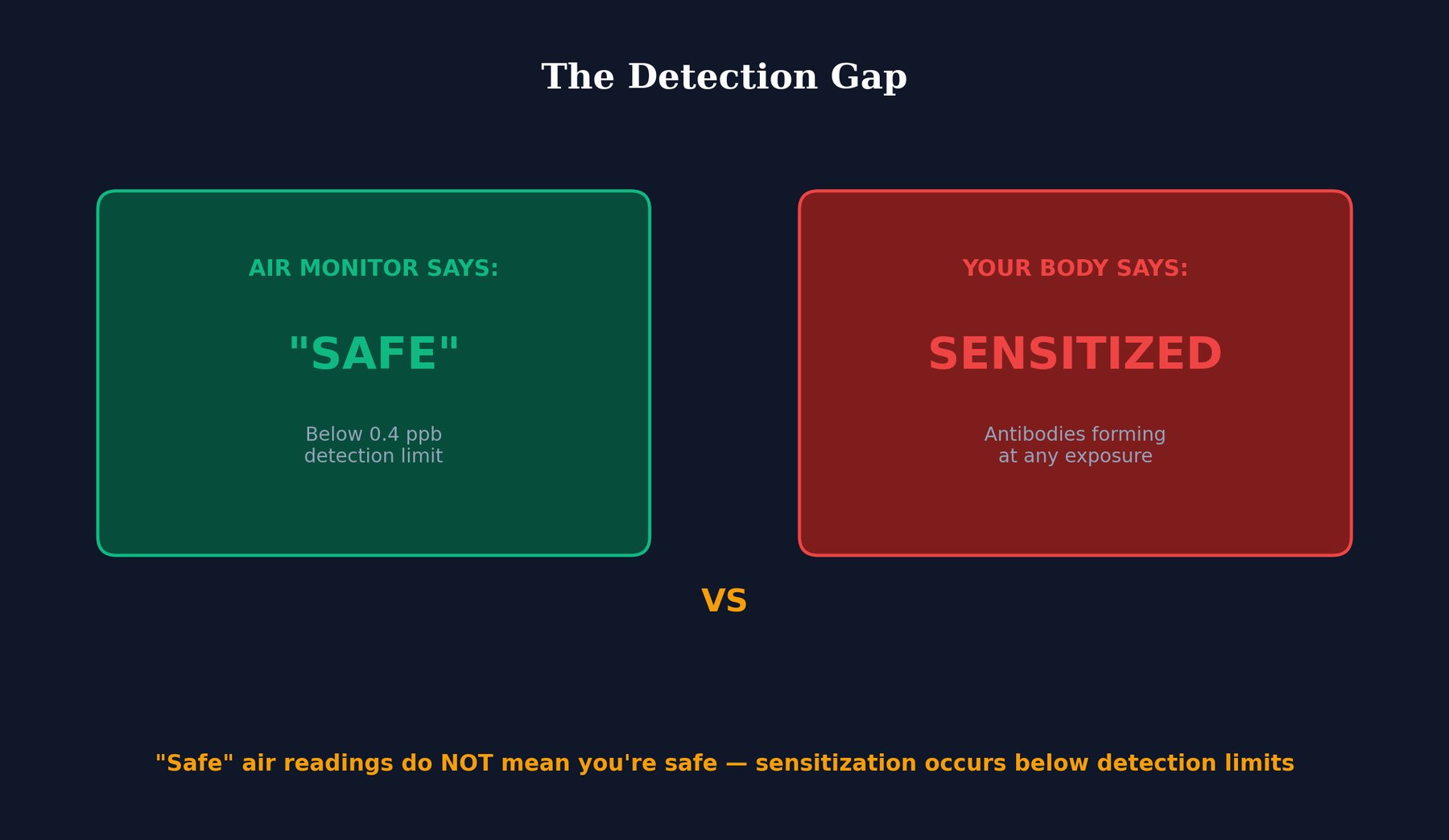
One of the most dangerous aspects of residential MDI exposure is that standard air quality monitors often fail to detect it, creating a false sense of security.
Detection Limits of Standard Monitors
Standard isocyanate air monitors (used by occupational safety agencies and industrial hygienists) have detection limits around 0.4-0.8 parts per billion (ppb). This means that if MDI concentrations are below these levels, the monitor will report "not detected" or "below detection limit."
Residential Off-Gassing Below Detection Limits
Residential off-gassing from improperly installed foam typically occurs at levels well below 0.4 ppb—often at 0.01 ppb or lower. This is intentionally designed in the foam formulation; residential foam isn't meant to off-gas at the high levels seen during and immediately after installation. But "low levels" doesn't mean "safe levels" for immune sensitization.
The Dangerous Interpretation
A homeowner (or their contractor) tests the air with a standard monitor, the monitor reports "not detected," and they conclude the air is safe. They move into or remain in the home. Meanwhile, their immune system is continuously exposed to sub-ppb levels of MDI vapor that the monitor cannot detect. Over weeks and months, sensitization develops silently.
Blood Antibody Testing: The Gold Standard
Air monitoring is unreliable for detecting residential sensitization risk. The gold standard is blood testing for MDI-specific IgE and IgG antibodies. If you've been exposed to chronic low-dose MDI and become sensitized, your blood will contain these antibodies even if air monitors show "safe" levels. However, most general practitioners and even many occupational medicine specialists don't routinely order these tests, so many cases of sensitization go unrecognized until a future MDI exposure triggers a severe reaction.
What This Means for You

If you have spray foam insulation that may have been improperly installed, or if you're considering spray foam installation, several critical points emerge:
Improperly Cured Foam Never Stops Off-Gassing
This is not a temporary problem that resolves after a few weeks. If foam was installed with incorrect mix ratio, wrong temperature, or equipment failure, the unreacted MDI remains in the foam indefinitely. The off-gassing can continue for months, years, or longer.
Sensitization Happens Silently Below Detection Limits
You may not feel sick. You may have no obvious symptoms. But your immune system may be developing sensitization to MDI based on continuous low-dose exposure that standard air monitors cannot detect.
Demand Proper Testing Before Installation
If you're planning to have spray foam installed, insist on:
- Professional installation by certified applicators with quality equipment
- Proper environmental conditions (appropriate temperature, humidity)
- Post-installation air quality testing with instruments capable of detecting sub-ppb levels
- Documentation of curing time and completion before reoccupancy
Blood Tests for Existing Exposure
If you suspect you've had chronic exposure to spray foam with improperly installed insulation, ask your physician about MDI-specific IgE and IgG antibody testing. These blood tests can determine whether you've been sensitized. If you have, your future occupational and environmental exposures must be managed carefully to avoid triggering severe allergic reactions.
Air Monitoring Alone Is Insufficient
An air quality report saying "MDI not detected" does not mean you're safe. It means only that current MDI concentrations are above the monitor's detection limit. For proper assessment of sensitization risk, blood antibody testing is gold standard.
Consider Removal If Improperly Installed
If you have documented evidence that foam was improperly installed and is continuing to off-gas unreacted isocyanate, removal may be the only truly effective remediation to prevent further sensitization.
Sources & References
- EPA Spray Foam Assessment and Guidelines
- Wisnewski et al.: Studies on MDI Sensitization from Occupational Exposure
- NIOSH Isocyanate Standards and Health Guidelines
- OEHHA Reference Exposure Levels for Isocyanates