Meet the Amine Catalysts
Spray foam insulation relies on amine catalysts to facilitate the chemical reaction that transforms liquid precursors into solid foam. The three main catalysts used in the industry are DMCHA (dimethylcyclohexylamine), DABCO (triethylenediamine), and BDMAEE (bis-dimethylamino ethyl ether). These volatile chemicals are trapped within the foam's matrix structure, but—critically—they are not chemically bonded to the foam itself.
This lack of chemical bonding means the amine catalysts slowly escape into the indoor air through a process called off-gassing. Unlike some components that fully integrate into the foam structure, these amines continue to volatilize for days or weeks after application, releasing vapor that permeates throughout the home. This off-gassing is not a sign of defective material; it's an inherent characteristic of how these chemicals function in the foam manufacturing process.
Blue Haze Vision: Understanding Glaucopsia
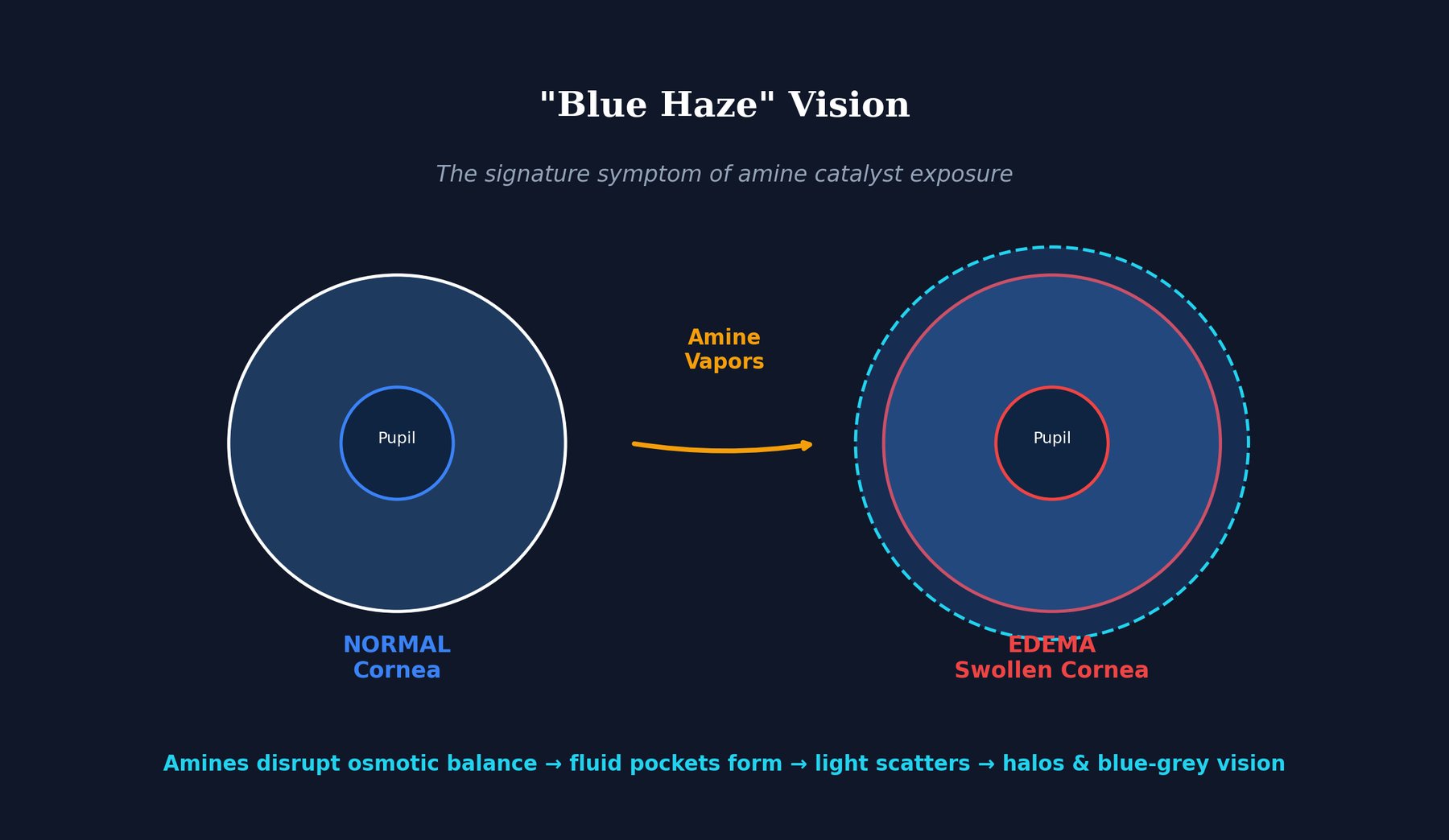
One of the most distinctive and alarming symptoms of amine catalyst exposure is glaucopsia—a temporary blue-grey haze that develops in vision when looking at bright surfaces or light sources. This unusual visual disturbance occurs through a specific physiological mechanism in the cornea.
When amine vapors contact the corneal epithelium (the outer layer of the eye), they disrupt the osmotic balance that normally maintains the cornea's clarity and structural integrity. This disruption causes fluid to accumulate within the corneal epithelium, forming tiny microcysts—microscopic fluid-filled pockets scattered throughout the corneal tissue. These microcysts scatter incoming light, much like fog particles scatter light and reduce visibility on a foggy day.
Individuals exposed to these amine vapors typically report seeing halos around lights, a distinctive blue-grey haze, and reduced contrast when viewing objects. These visual symptoms are usually reversible—once exposure ceases and the amine vapors clear from the environment, the corneal edema resolves within days to weeks as the osmotic balance restores.
However, this reversibility has limits. Prolonged or repeated exposure to high concentrations of amine vapors can cause more persistent corneal damage, including scarring and chronic changes that may not fully resolve. The appearance of blue haze is essentially an early warning system—the eye is signaling that amine concentrations have reached damaging levels.
The Health Effects Cascade
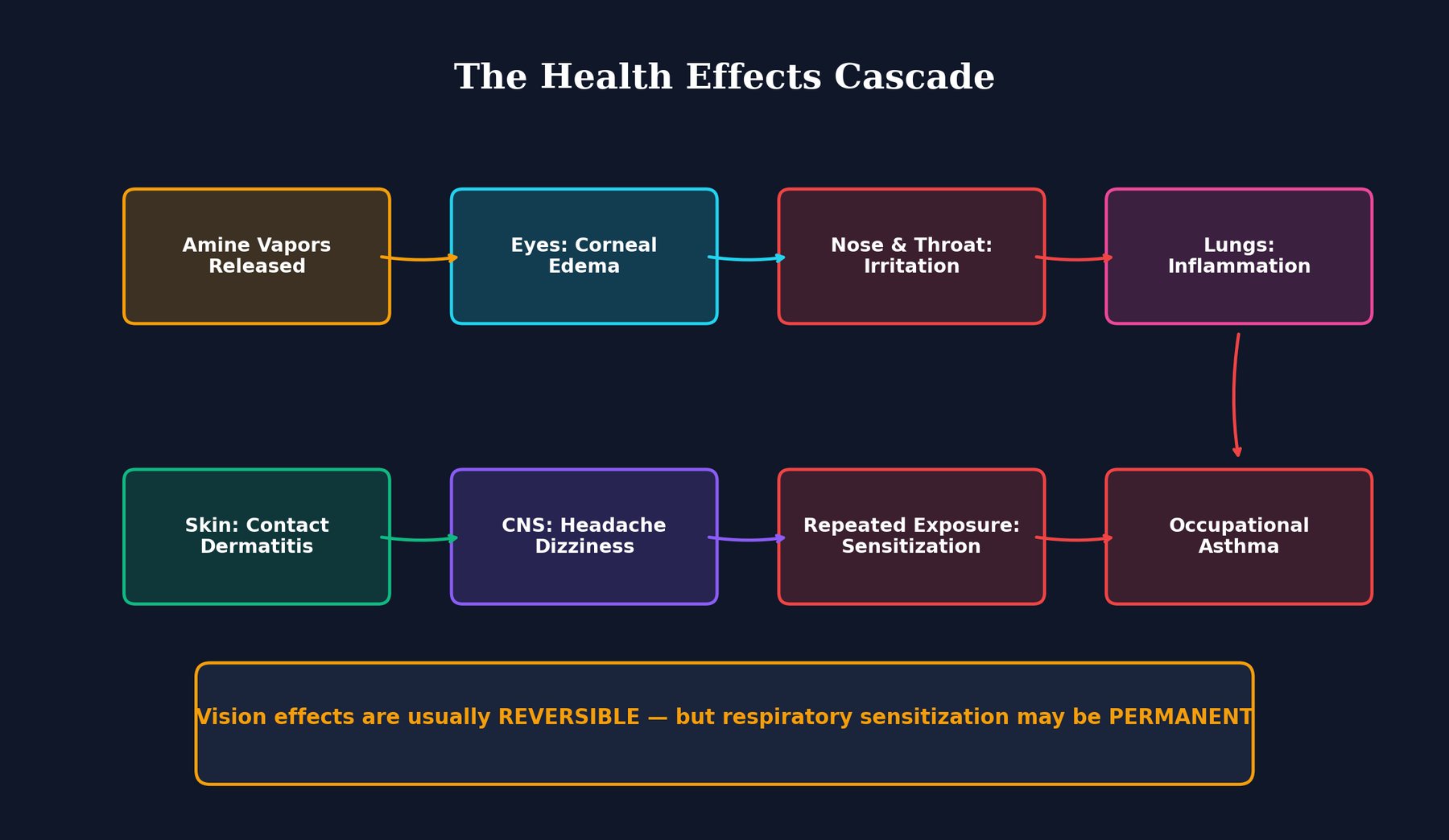
Amine catalysts attack multiple body systems through a cascading pattern of exposure and response. As amine vapor spreads through the home, different tissues and organs respond based on their exposure route and chemical sensitivity.
Eyes: Corneal Edema
As discussed, amine vapors cause corneal edema and glaucopsia. This is typically the first symptom to appear because the eyes are directly exposed to the gas.
Respiratory System: Burning and Inflammation
Amine vapors are water-soluble and readily dissolve in the mucous membranes lining the nose and throat, causing burning sensations, inflammation, and discomfort. This irritation extends down into the lungs, where amine exposure triggers inflammatory responses in the airways and alveoli. Individuals report coughing, difficulty breathing, and chest tightness.
Skin: Contact Dermatitis
Direct contact with uncured foam or amine-contaminated surfaces causes contact dermatitis—redness, itching, and inflammation of the skin. Workers handling foam without adequate protective equipment commonly experience this reaction.
Central Nervous System: Headaches and Dizziness
Amine vapors can cross into the central nervous system, causing headaches, dizziness, and neurological symptoms. Some individuals report brain fog and difficulty concentrating during acute exposure periods.
Respiratory Sensitization: The Long-Term Threat
With repeated exposure, the immune system can develop sensitization to amine catalysts. This means the body's defenses treat the amine as a foreign invader and mount an allergic-type response. Once sensitized, even very low concentrations of amine vapor trigger symptoms. This sensitization can progress to occupational asthma, where exposure consistently triggers airway constriction, wheezing, and breathing difficulty.
Critically, respiratory sensitization is often permanent. Even years after the foam installation, if amine vapor is encountered again, the sensitized individual will experience an immediate asthmatic response. The initial vision effects are reversible, but the respiratory effects can be permanent.
Off-Gassing Timeline: When It's Safe to Return
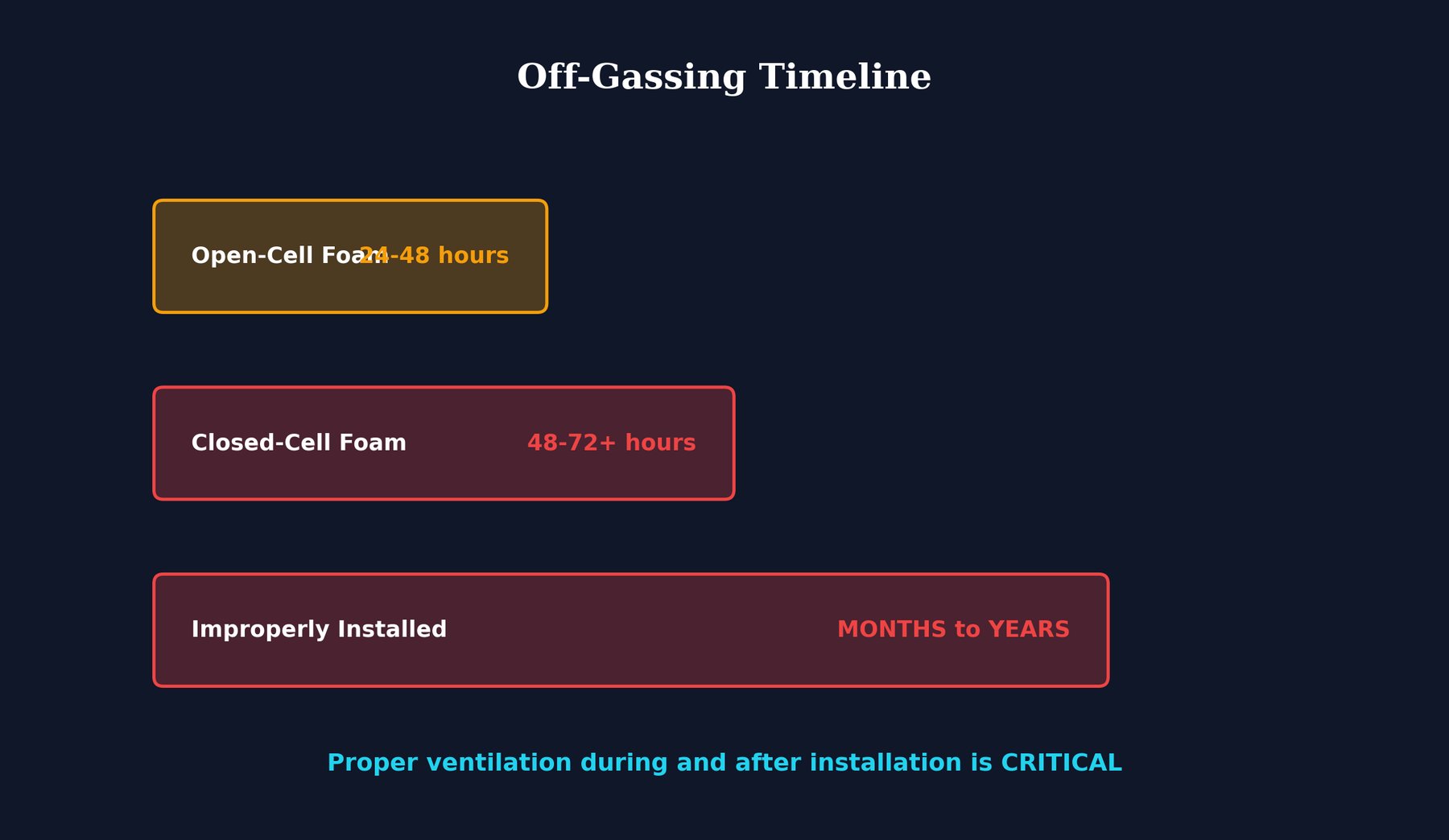
The duration of amine off-gassing varies significantly based on foam type and installation quality:
Open-Cell Foam
Open-cell foam has large interconnected pores and a lower density. Amine catalysts have easier access to the surface and escape more rapidly. Typically, the worst off-gassing occurs within the first 24-48 hours after installation. By 48 hours, amine concentrations generally drop to levels that most people can tolerate, though some individuals with heightened sensitivity may experience symptoms for longer.
Closed-Cell Foam
Closed-cell foam has smaller, isolated pores and higher density, creating more barriers for amine vapor to escape. Off-gassing is more prolonged, typically continuing at significant levels for 48-72 hours or longer. The denser structure means amines trapped deep within the foam take substantially longer to reach the surface and volatilize.
Improperly Installed Foam
When installation parameters are incorrect—wrong application temperature, humidity, mix ratio, or equipment malfunction—the foam may not cure properly. Incompletely cured foam continues off-gassing for weeks, months, or even longer. In some cases, improperly installed foam becomes a chronic source of amine vapor for years.
Recommended Evacuation Period
Industry recommendations and health guidance suggest evacuating the treated space for at least 24 hours for open-cell foam and 72 hours for closed-cell foam. For homes with improperly installed foam, longer evacuation may be necessary, and additional testing may be warranted before reoccupancy.
- Open-cell foam: 24-48 hours minimum
- Closed-cell foam: 72+ hours minimum
- Improperly installed: Longer evacuation and air quality testing recommended
What This Means for You
If you're planning spray foam insulation or suspect amine exposure in your home, several practical conclusions emerge from the science:
Blue Haze Is Your Early Warning System
If you or family members develop blue-grey haze vision, halos around lights, or other visual disturbances during or shortly after foam installation, this is your body signaling significant amine exposure. Do not ignore this symptom—it indicates vapor concentrations have reached damaging levels.
Respiratory Sensitization Is the Bigger Long-Term Risk
While corneal edema and acute symptoms are uncomfortable, respiratory sensitization poses a more serious long-term health burden. If you develop asthma or respiratory symptoms after foam installation, seek medical evaluation and consider antibody testing to determine if you've been sensitized. A permanent sensitization will affect your health and quality of life far longer than temporary vision effects.
Ventilation Is Essential
Ensure the building is thoroughly ventilated for the full recommended period—24-72 hours depending on foam type. This means opening windows, running exhaust fans, and maintaining air exchange even in winter or summer. Do not rely solely on HVAC systems that may recirculate contaminated air.
Stay Out During Installation
Occupants and pets should not be present during foam application or for the recommended post-installation period. The first hours after installation are when amine concentrations peak. Temporary displacement is the most effective protection.
Monitor Your Health
If you develop persistent respiratory symptoms, asthma, or other health changes after foam installation, report them to a medical provider and mention the spray foam exposure. Occupational/environmental medicine specialists can order antibody testing to assess whether sensitization has occurred.
Sources & References
- CDC: Health Hazards of Tertiary Amine Catalysts
- CPSC Staff Review: Spray Foam Insulation
- JAMA Ophthalmology: Amine-Related Vision Disturbances